
☛ Cette chronique est aussi disponible en français [➦].
Translated by Florence Bois-Villeneuve.
To know more about Les 3 sex*’s editorial policy and text selection process, click here.
This text was written by two people who suffer from endometriosis. As endometriosis sufferers, not only do we live with its physical and psychological effects, but also the myriad of challenges related to its management and the lack of awareness about it.
Endometriosis is characterized by the abnormal presence of endometrial tissue—or uterine tissue, also known as the endometrium—outside of the uterus. The amount of tissue varies according to menstrual cycles and the effects of sex hormones (Inserm, 2018). The tissue growth is considered pathological when it causes pain and/or compromises the fertility of the person affected.
From the first signs of puberty, between 10 and 15% of people with a uterus are reported to be affected by endometriosis (Nisolle et al., 2007).
In recent years, endometriosis has been increasingly documented, paving the way for more effective, albeit still inadequate, medical treatments. Even today, in Canada, endometriosis can take an average of six years to diagnose (Singh et al., 2020). Endometriosis is a multifactorial disease arising from the combined action of genetic factors and possibly environmental factors (Haute Autorité de Santé, 2017).
The lesions caused by endometriosis are mainly located in the pelvic cavity, but can also become lodged in the abdominal cavity, on the diaphragm, and more rarely in or around the chest cavity. Deep pelvic endometriosis lesions mainly affect the uterosacral ligaments, posterior cul-de-sac, bladder, rectum, ureters, colon and digestive tract (Haute Autorité de Santé, 2017).
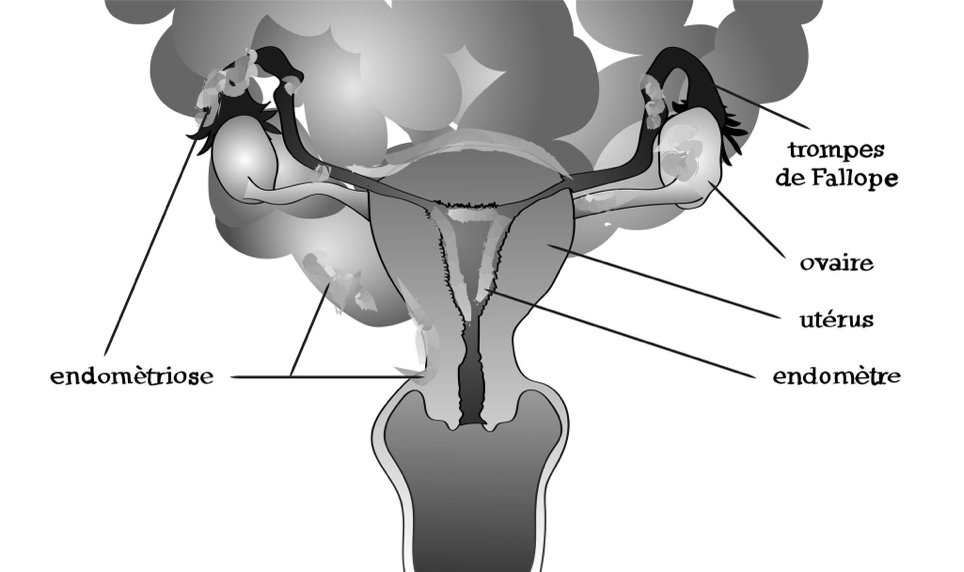
Photo credit: Mona Chancogne
Diagnostic challenges
Historical background
According to radiologist and endometriosis specialist Érick Petit (2016), clinical descriptions of a condition resembling endometriosis can be found in ancient medical writings, notably in the work of Hippocrates (4th century CE) and Plato (5th-4th centuries BCE). While the symptoms themselves do not appear to have changed—“violent uterine contractions, inflammation, syncopal events or seizure throughout [said] woman’s life” (Petit, 2016, p. 21)—the interpretations of these symptoms have evolved considerably.
In Europe, in the Middle Ages and up to the Classical period (17th-18th centuries), these symptoms were regularly discredited and considered by scientists to be related to a form of hysteria or possession (Petit, 2016). In the 19th and 20th centuries, the symptoms were dismissed as nature’s way of punishing women who had put their careers ahead of motherhood (Čapek, 2010). Finally, in the 20th century, these symptoms were perceived as arising from women’s troubled relationship with their femininity, their supposed fragility, and their “deviant” sexual behaviours (Montgomery, 1994).
Far from the “objective” and “neutral” aims of medical science, the fear and discomfort evoked by these symptoms instead fuel a policy of exclusion of women, stigmatizing them as mad or excessive.
Clinical symptomatology
People with endometriosis may be symptomatic or asymptomatic. There are as many different forms of endometriosis and manifestations of symptoms as there are people who suffer from the condition. However, the clinical signs most often reported are the following (Nasir and Bope, 2004; Bazot et al., 2009):
- Dysmenorrhea: intermittent cramps linked to the menstrual cycle (lasting approximately 24 to 72 hours). The pain may radiate to the back, thighs, lower back, and suprapubic area;
- Deep dyspareunia: persistent pain during or after intercourse;
- Pain on defecation: alternating diarrhea and/or constipation;
- Non-cyclical pain: pain at times other than during menstruation;
- Infertility: reproductive problems (difficulty conceiving, maintaining a viable pregnancy, or carrying to term);
- Asthenia: chronic or temporary fatigue;
- Dysuria: pain when urinating.
There are many comorbidities that are invisible but are often linked to the disease: depression, headaches, sexual dysfunction (pain during intercourse, anxiety about impending sexual relations, low libido), chronic fatigue, bloating, vomiting, palpitations (Haute Autorité de Santé, 2017). While some of these symptoms are common to all people with endometriosis, infertility tends to monopolize the media discourse, painting reproduction as the central health concern for people assigned female at birth (Čapek, 2010).
This sheds light on a harmful trend towards essentialism, making endometriosis an attack on “femininity.” Marion Coville, who is non-binary, points this out in their article on endometriosis, in which they explain that, by focusing solely on the female and maternal experience of this disease, the media constantly pigeonhole sufferers as having a stereotypical “women’s disease.”
“The [magazine] articles that I read define a version of “femininity” that is made up of the uterus, the desire to be a mother, heterosexual relationships, and the possibility of being penetrated, and offer up advice on how to “stay womanly,” “despite everything.” (Coville, 2018, p. 22).

Photo credit: Mona Chancogne
While these considerations explicitly refer to an essentialist understanding of “femininity,” they also contribute strongly to marginalizing the medical care of individuals who, if not cisgender women, have a uterus. A battle is still being waged on two fronts: the battle to have endometriosis recognized as a disease, and the battle to give substance to “a queer experience of endometriosis” (Coville, 2018, p. 22).
Diagnosis and treatment
When patients consult a medical professional for their symptoms, very often their suffering is trivialized, to the point they are even blocked from obtaining a diagnosis. Yet the presence of pain is the first major warning sign (Haute Autorité de Santé, 2017, p. 123). But then there’s the famous “it’s all in your head,” the all-too-common dismissal and psychologizing of the menstrual pain reported by sufferers (Denny, 2009; Čapek, 2010).
In the presence of endometriosis symptoms, health practitioners perform a targeted gynecological exam, including examination of the posterior cul-de-sac, and an assessment of the pain and/or the analgesic effect of a treatment, accompanied by a radiological examination, if necessary (Haute Autorité de Santé, 2017; Leyland et al., 2019). A pelvic examination (with speculum) can reveal various clinical signs, such as bluish vaginal lesions, painful nodular lesions on vaginal or rectal exam when posterior involvement is suspected, or a retroverted uterus (Riazi et al., 2015).
Doctors are also recommended to prescribe combined oral contraceptives (to regulate periods) or progestins (other hormones that do not necessarily have a contraceptive effect) (Leyland et al., 2019). If these treatments fail, more substantial hormonal treatments may be recommended, such as GnRH agonists (which induce a sort of artificial menopause). If all these solutions fail, the patient may be referred to an obstetrician-gynecologist for laparoscopic surgery (Leyland et al., 2019). During the procedure, the endometriotic lesions are either burned off or cut out (Hidaka et al., 2012). Following this procedure, patients are often advised to continue taking hormones (Falcone and Flyckt, 2018).
In Canada, laparoscopy is the only way to diagnose endometriosis. However, even if this surgery leads to an overall reduction in symptoms in the short term, it does not necessarily solve the problem, and it is often necessary to have the surgery more than once. This procedure can even be counterproductive in the long term, as stimulating the endometriotic tissue can ultimately cause the endometriosis to spread (Abbott et al., 2003).
In fact, medical treatments, which may attempt to control menstrual flow or estrogen levels to prevent the so-called spread of the endometriosis, can only be considered short term. More invasive treatments can destroy excess tissue. However, there are no curative treatments to speak of (Leyland et al., 2019). Yet, the issue of sufferers’ overall and sexual quality of life is hardly ever addressed (Barbara et al., 2017).
A feminist analysis
One feminist critique could highlight the fact that clinical descriptions of endometriosis are still based on knowledge formulated by the dominant classes of a medical system that is, to this day, controlled by the heteropatriarchy. In any case, it is astonishing how long this disease has been invisible—and how blatantly it has been denied. For a long time, the authorized discourse failed to consider—or take seriously—the subjective experience of a certain number of people, for the sake of protecting a hierarchy of knowledge as well as “experts.”
This denial is at the root of a veritable “production of ignorance” in terms of an understanding of the disease, the diagnostic and treatment methods, and patient care.
The “production of ignorance””is an epistemological concept proposed by philosopher Nancy Tuana, a leading figure in critical and feminist epistemologies of ignorance (Verburgt, 2020). She demonstrates that many subjects of study concerning women’s bodies (genitalia, sexual pleasure, etc.) have been ignored by the medical field.
An analysis of this phenomenon led many epistemologists to consider ignorance not as a lack (which science could simply fill) or an absence of knowledge, but as an active construction, built and placed in service of social and political interests (Verburgt, 2020).
Our criticism of endometriosis could just as easily apply to polycystic ovary syndrome, vaginismus or vestibulodynia.
“Practices of ignorance are often intertwined with practices of oppression and exclusion” (Tuana, 2006, p. 1).
In this case, we might consider standpoint theory or standpoint epistemology, a theory that cleverly reminds us that knowledge always stems from a position, which can be situated in terms of the grammar of social, ideological, cultural genders, etc. (Harding, 2004). From these reflections emerge the legitimacy and the need, not only to understand the position from which discourses are produced, but also and above all to integrate into the learning process the knowledge of those concerned, i.e., the people who are affected by the phenomenon being studied.
As a result, patients are often perceived by practitioners as untrustworthy and are relegated to the status of subjects devoid of knowledge and agency (Tuana and Sullivan, 2006). To cope with being excluded from the field of knowledge and therapy related (ironically) to their own conditions, patients took matters into their own hands. They have developed self-help practices, for example, by publishing books such as Our Bodies Ourselves (Cresson, 2016), and by forming support groups with the goal of sharing tools and information and creating spaces for supportive dialogue aimed at alleviating their suffering (Haute Autorité de Santé, 2017, p. 117).
PRACTICAL MANUAL AND RESOURCES
To conclude, we will propose a set of resources and tools that have helped us in our own journeys with endometriosis:
1. Existing resources for a safe diagnosis
Patients often dread gynecology appointments (Quennehen, 2020). They may be embarrassed to show their body to a stranger or to have an exam during their period. This discomfort may also stem from a general unfamiliarity with what happens during gynecology appointments or a fear of the potential attitudes of health professionals (Quennehen, 2020). Finally, patients mainly associate the pelvic exam with feelings of humiliation, inferiority, anxiety, and incomprehension about the procedure (Westhoff et al., 2011).
People who receive gynecological care may also experience gynecological violence (or abuse). Gynecological and obstetrical violence can be defined as “gestures, comments, practices and behaviours carried out or omitted by one or more members of the care staff on a patient during their gynecological and obstetrical follow-up” (Bousquet et al., 2018, p. 32).
This violence (or abuse) can take many forms, from psychological violence (withholding information, sarcastic or judgmental comments) to physical violence, verbal violence and even sexual violence (Bousquet et al., 2018; Cardenas Castro and Salinero Rates, 2021). Because gynecologists can inflict this violence unintentionally, you are well within your rights to perceive how you were treated as abnormal.
There are many resources that can help you to have a safer care experience. Some compassionate health professionals out there have a positive, anti-oppressive and/or feminist practice; the Gynéco Positive site can help you find one.
There is also the book S’armer jusqu’aux lèvres : quelques outils d’auto-défense gynécologique à l’usage de toutes les femmes* [Armed to the lips: some gynecological self-defence tools for every woman], which could help you develop some gynecological self-defence techniques.
2. Alternative or additional solutions
The next section is largely based on personal experience. While the effectiveness of some of the treatments and practices below has not been demonstrated in a systematic, biomedical manner, these alternatives have been helpful for some people. Before anything else, Les 3 sex* strongly encourages you to consult a health professional.
Some alternatives can help to control the pain and other symptoms:
- Apply topical clays (Nissim, 1997);
- Eat an anti-inflammatory diet: avoid gluten, dairy products, tea, coffee, alcohol, red meat and sugar (Grisel and Bayard, 2020);
- Avoid endocrine disruptors in cosmetics, cleaning products, etc.;
- Drink raspberry, lady’s mantle or yarrow tea (ask an herbalist for advice) (Nissim, 1997).
Electronic devices:
- Use a transcutaneous electrical nerve stimulation (TENS) machine (purchased online or at a pharmacy) (Mira et al., 2015), a non-invasive device used to relieve pain in various parts of the body.
- Use an electric hot water bottle (for continuous heat) or a regular hot water bottle.
Specialties to consider:
- Acupuncture: Practice originating in Chinese medicine that involves inserting needles at precise points on the surface of the body to treat various illnesses or provide pain relief;
- Visceral osteopathy: The application of manual therapy techniques to the inner organs to improve function (indexsante, 2015);
- Sophrology: A relaxation method based on hypnosis and relaxation;
- Hypnotherapy: A form of alternative medicine that uses hypnosis for therapeutic purposes, in particular to treat pain;
- Phytotherapy: The treatment of illnesses using plants or their extracts;
- Psychotherapy: The practice of “assessing psychological and mental functioning, and determining, recommending and carrying out interventions and treatments to promote psychological health and restore the mental health of human beings in interaction with their environment” (Ordre des Psychologues du Québec, 2020).
Practices:
- Yoga: Physical and philosophical practice that consist in performing a set of postures and breathing exercises to improve physical and mental well-being (Gonçalves et al., 2017);
- Mindfulness meditation: A Buddhist-inspired practice of bringing attention back to the present moment (present actions and sensations), used to reduce stress and anxiety. Mindfulness meditation is based on breath control.
Apps:
- Easy endo (free): Provides information on treatments, a symptom tracker, endometriosis news, a discussion forum, and experts available once a month to answer specific questions;
- Luna (paid): Helps to track, assess and analyze pain, sexuality and quality of life. Offers personalized advice, educational content, questions and answers;
- Nabla (free): Features a content library written by health professionals;
- Vulvae (paid): A tool for tracking positive or negative factors (daily habits, personal hygiene, sexuality, mood, treatments) related to vulvar health. Information and tools to prepare for medical appointments. Pain management programs are also offered.
You will also find a wealth of relevant information on the following endometriosis websites:
- Endométriose Québec: Québec organization dedicated to supporting sufferers and sharing information about the disease.
- Endofrance: French association dedicated to sharing reliable information about endometriosis.
- Endoqueer: Organization dedicated to sharing information about endometriosis from a queer perspective.
Comments